
can an overshot jaw correct itself free sample

This website is using a security service to protect itself from online attacks. The action you just performed triggered the security solution. There are several actions that could trigger this block including submitting a certain word or phrase, a SQL command or malformed data.
This website is using a security service to protect itself from online attacks. The action you just performed triggered the security solution. There are several actions that could trigger this block including submitting a certain word or phrase, a SQL command or malformed data.

Foals with an overbite, commonly called a parrot mouth, have upper incisors that protrude past the lower incisors. While some breeders droop their shoulders and shake their heads when faced with affected foals, floundering in their misfortune, others pick up the phone and call the equine orthodontist.
Parrot mouth, long believed to be an inherited condition, reportedly affects 2-5% of the equine population to some degree. Although common in other species, like humans, any degree of overbite is considered abnormal in horses.
“Other animals with an overshot jaw have difficulty grasping food because of misaligned incisors. In horses, incisor malalignment is obvious but not necessarily a significant problem, because they are capable of seizing food with their lips. The major concern is the potential development of cheek-teeth disorders that inhibit their ability to chew,” shared Kathleen Crandell, Ph.D., an equine nutritionist for Kentucky Equine Research.
Foals with an overshot jaw are therefore at risk of malnutrition, slow growth, and the development of additional dental problems. For example, lack of contact between the upper and lower incisors can result in overgrowth of incisors and cheek teeth, known as premolars. In addition, this lack of contact may trap the lower incisors behind the upper incisors, potentially contributing to the lack of lower jaw growth, which exacerbates the condition as the foal grows.
According to a recent study*, tension band wires on the upper dental arcade either with or without the use of a bite plate on the floor of the mouth, under the tongue, successfully corrects or improves the condition. Researchers reported the following observations from the study:
“Despite these positive results, owners should be aware that treated foals require skull radiographs, at least two surgical procedures performed under general anesthesia, and may have post-treatment complications,” warned Crandell.
Such complications include facial-nerve injuries, irritation to the mare’s udder during nursing, and discoloration and abnormal growth of the incisors.
In addition, it may not be ethical to breed animals with corrected bites, considering parrot mouth is strongly believed to be an inherited unsoundness.

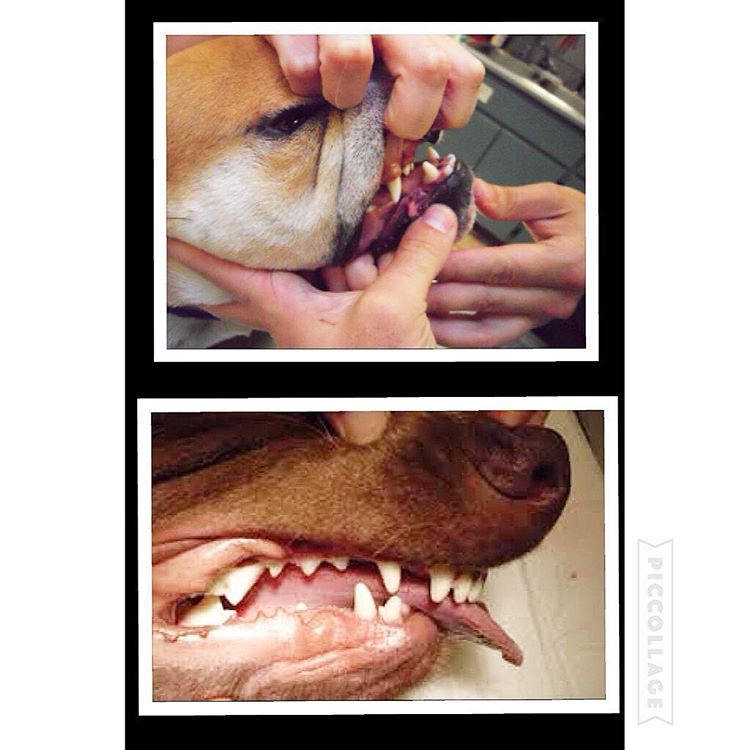
Here is a visual look into what an “undershot” and “overshot” jaw looks like. In recent years, I’ve noticed more and more dogs with this issue. Can a dog live productive life with a malocclusion: (imperfect positioning of the teeth when a jaws closed) Yes but with some issues along the way.
Let’s begin with a puppy will have 28 “puppy teeth” by the time it reaches six months old (this number can vary from breed to breed) By adulthood, most breeds will have a total of 42 teeth. As defined above a malocclusion or simply a misalignment of a dog’s teeth occurs when their bite does not fit accordingly beginning as puppy’s teeth come in and worsening as their adult teeth follow.
the upper jaw is longer than the lower one, an overshot or overbite. When a dogs mouth is closed, a gap between the upper and lower incisors (teeth) will be present. In most cases, puppies are born with a slight over/under bite and with time the problem can correct itself if the gap is not too large. What should be noted is if a dog’s bite remains over/undershot by 8-10 months old, that’s how it will remain for the remainder of its life. In overbite’s the structure may worsen as the permanent teeth come in as they are larger and can damage the soft parts of the mouth. Teeth extractions are sometimes necessary.
Structural dentition of a puppies jaw should be checked very early on to help eliminate this issue. Unfortunately most dog owners won’t notice until is late in the game. More so is the issues of backyard and/or inexplicable breeders breeding dogs with undershot/overshot jaws and potentially passing along this trait to future generations.
With an overbite, the upper jaw is longer than the lower one. When the mouth is closed, a gap between the upper and lower incisors occurs. Puppies born with an overbite will sometimes have the problem correct itself if the gap is not too large. However, a dog’s bite will usually set at ten months old. At this time improvement will not happen on its own. Your pet’s overbite may worsen as the permanent teeth come in because they are larger and can damage the soft parts of the mouth. Teeth extractions are sometimes necessary.
Problems that can arise from malocclusion are; difficulty chewing, picking up food and other objects, dogs with overshot jaws tend to pick up larger chunks of food since they can’t chew nor pick up smaller morsels which can lead to choking and future intestinal issues. These dogs are also prone to tartar and plaque build up which if left untreated can lead to other significant health issues such as heart problems. Other issues are listed below:
What’s important to note is that most malocclusions do not require treatment, it’s simply how a dog will live its full life as. This is important since most breeders breeding for financial gains don’t think about. What can be done is to brush the teeth regularly to prevent abnormal build-up of tartar and plaque. A veterinarian in cases that can be solved will sometimes recommend a dental specialist if a client want to correct the teeth misalignment. Recently I’ve heard o specialist putting “braces” on puppies to realign the teeth.
#dog #dogs #puppy #pup #puppies #puppylove #pets #life #family #bulldog #maltese #mastiff #chihuahua #cockerspaniel #vet #meds #instadog #instagood #instadaily

A dog"s bottom jaw will continue growing until the age of 10 - 12 months. Until this time a slight undershot will often correct itself naturally with ageing. A severe overshot is unlikely to correct itself but is not a significant health issue for the dog. Overshot dog"s can still lead healthy lives as happy and loving pets regardless of this problem. Dog"s with an overbite should not be shown or bred from.UNDERSHOT BITE:also referred to as an underbite. This when the bottom jaw is longer than the top jaw and the incisors on the bottom jaw protrude past those of the top jaw. This type of bite is actually correct for breeds such as the bulldog. An underbite generally does not adversly effect the dog in anyway. These dogs still make loving and healthy pets but should not be shown or bred from.LEVEL BITE:also called the pinscer bite. This is where both jaws are the same length and the incisors meet edge to edge. This bite does not affect the dog adversely in any way but can cause premature wearing of the incisor teeth. Often in a slightly older dog the bite can go from scissor to level with ageing.WRY BITE:This is where the bottom jaw is twisted and the incisors do not meet in a correct straight scissor bite. This type of bite is not very common and generally the dog suffers no ill effects. A dog with a wry mouth should not be shown or bred from.
In most cases and overshot, undershot, level or wry bite is not a serious condition and should not discourage someone from purchasing such a pup unless their intentions are specifically to show or breed. In the wild a dog with an incorrect bite could have great difficulty hunting and killing prey. For the purposes of a pet an incorrect mouth is not a serious concern as modern prepared dog foods are in palatable sized portions. An incorrect bite would however exclude a dog from a working career where the dog was required to use it"s mouth, for example, herding or police work.BITE GENETICSThe inheritance mode of a dog"s bite is largely unknown and litters may present with confusing outcomes. However, because an incorrect bite can be determined by 12 months of age, a dog with such a fault can be excluded from a breeding programme.
Incorrect bites vary greatly with respect to severity and occurrence. Some breeds and lines within breeds appear to have a higher incidence of bite faults than others. It has also been found that dogs with undershot bites often result from parents with correct scissor bites. This would indicate that the fault is recessive but no conclusive proof is available.
Dogs who produce offspring with bite faults should not necessarily be exclude from a breeding programme because of this reason alone. There is a saying, "Don"t throw out the baby with the bathwater." Which basically means that a good example of the breed both in conformation and temperament should not be excluded solely because it has produced offspring with an incorrect bite. Other offspring from this dog may be perfectly correct in mouth. To exclude such a dog would mean eliminating valuable genetic material from the population unnecessarily. To breed from this dog would however mean that the fault can not be eliminated completely from future generations and as such the offspring would need to be checked for this fault. Often a recessive fault can go unseen for several generations before it makes an appearance again.
It has also been suggested that the bite might not be entirely governed by genetics and that the size of the actual incisors can play a role in the bite. In our own breeding programme we have observed that dogs with larger incisors are less likely to have an even or overshot bite as an older dog.
Because the bottom jaw continues to grow until the dog reaches 12 months is has been observed that a puppy with a slight overshot bite has corrected. Hence it is sometimes worth retaining an otherwise promising puppy that may have a very slight gap in the jaws at a young age. Some people say that a matchstick gap is ideal. Puppies with smaller incisors and no gap can actually go even or undershot. Some breeders also believe that a slight overshot can be corrected by administering the puppy extra calcium supplements at a young age while the jaw is still growing.
A bite can stay the same throughout puppyhood or change greatly as the dog grows during the first year. There is no hard and fast rule. We have observed a particular puppy go from being overshot to scissor to even to undershot in the space of several months while it"s littermates held perfect scissor bites the whole time.MISSING TEETH (incomplete dentition)Another concern from a breeding perspective is dogs that have missing teeth. For most working and herding breeds the standard requires full dentition (42 teeth).
Once again the genetic mode of inheritance for missing teeth is unknown. Parents with full dentition can produce offspring with one or more missing teeth suggesting inheritance is recessive. This appears to be compounded by the fact that x-rays have shown that some dogs who were thought to have a missing tooth, actually possessed the tooth in question but it was below the gum-line and was therefore not visible.
Some breeders are overly pedantic about a dog having one missing tooth and will eliminate such a dog (and even sometimes it"s parents) from their breeding programme. This action is unwarranted as the genetic material in an otherwise excellent specimen could be lost forever. This decision can be yet another example of "Throwing out the baby with the bathwater." Particularly when the mode if inheritance is not understood.
Although missing teeth are certainly not desirable in a show or breeding dog, there are very few standards that actually describe this as a serious or disqualifying fault (one of which is the German Shepherd Dog). The ANKC standards for the Australian breeds do not state that full dentition is required therefore although not desirable, a dog should not be penalised for having a missing tooth.MOUTH HEALTHA puppy"s teeth and bite should be regularly checked whilst they are growing. This is to ensure that the bite is correct but also to make sure that the deciduous teeth fall out correctly as the permanent teeth grow in. It is possible for a puppy to retain baby teeth particularly the canine teeth (this is quite common in smaller breeds). These teeth will need to be pulled or removed if they don"t fall out naturally. Sometimes the tooth is already loosened by the permanent tooth and can just be wiggled and will come free. It the tooth is still deep rooted and not loose it may need to be removed by a veterinarian.
When puppies are teething their gums are often sore and swollen. It is of value to supply the puppy with something suitable and safe to chew which will both help relieve the discomfort and loosen the deciduous teeth. Brisket bones and rawhide chews are ideal.
Overall gum and tooth health requires the owner to periodically check the teeth for build up of tartar or any infections. A dog"s teeth need to be checked just like humans do. It is also worth mentioning that a diet of only soft foods is not good for tooth health.

infects the mother during pregnancy. If these organisms or substances reach the fetus at the appropriate time during gestation, defects and abortions can

My baby is 4.5 months old, and alas, still has the overbite. She had a perfect sizzors bite when I picked her up, and I noticed that around 11 weeks old, she started to get an overbite.
As I said, she did have a good bite at 6-11 weeks old, but she hit the 11th week and it started to develop. None of her litter mates have an overbite...
Krista, the lower jaw grows at a rate different from the muzzle. A puppy can have a perfect scissors bite, then this can change briefly from this to an overshot or even an undershot lower jaw. The muzzle can suddenly grow very quickly in length and the lower jaw has to catch up.
I"m taking her into the vet tomorrow, see what they think, and I"ll report back, good or bad news. THANKS FOR ALL OF THE HELP AND THE PERSONAL EMAILS! THANKS
I can"t find the previous thread, I didn"t realise it was so large... if your pup has a really large overbite of 1/2" or more there might be a problem. I think that is kind of alot, and you definately need to watch whats going on with her canines. Let us know what your vet said.
Still alot but hope it keeps on getting better. I have seen a couple dogs like this over the years but neither one ever corrected itself back to a correct bite.

There are many different designs of functional appliances. These can be removable plates or fixed appliances with piston-type arms. The vast majority are used to correct incisor protrusion in the growing child, especially where the bottom jaw is undershot (Class II Division 1 malocclusion).
Although the design and wear of these appliances differ, the aim of treatment and essential action is quite similar. They have to be worn a minimum of 12 hours per day, mainly at night. Treatment time can take up to 12 months, including a retention phase where the appliance wear is gradually eased off.
Undershot is a class III malocclusion that is also referred to as mandibular prognathism, maxillary brachygnathism, mandibular mesioclusion, or an underbite. This malocclusion is characterized by a shorter upper jaw and a longer lower jaw, resulting in lower teeth that are in front of the upper teeth. While this condition is normal for some breeds, such as Bulldogs, in many breeds it is unusual. An undershot jaw occurs when the lower jaw grows faster than normal and becomes longer than the upper jaw, and is usually evident around 8 weeks of age in puppies. This misalignment can cause soft tissue trauma, such as to the lips. When the incisors meet instead of fitting next to each other, it is called a level bite. When the malocclusion causes the lower incisors to be placed in front of the upper incisors, it is called a reverse scissors bite.
The cause of overshot and undershot jaws in dogs relate to the increased or decreased rate of growth of the upper and lower jaws in relation to one another. This can occur due to a: Genetic disorder Trauma; Systemic infection ;Nutritional disorder; Endocrine disorder; Abnormal setting of puppy teeth; Early or late loss of puppy teeth.
After a quick physical exam, your vet may have to sedate your dog in order to perform a thorough oral exam. This will assess your dog’s skull type and teeth location in relation to the teeth on the opposite jaw. Often, the placement of the upper and lower incisors in relation to one another can determine what type of malocclusion your dog has. Your vet will note any areas of trauma due to teeth striking those areas, and any cysts, tumors, abscesses, or remaining puppy teeth that may be present. A dental X-ray can also help to assess the health of the jaws and teeth. These diagnostic methods will lead to a diagnosis of an overshot or undershot jaw in your dog.
Treatment of a jaw misalignment will depend on the severity of the condition. If your dog has a misalignment, but can still bite and chew food without problems, no treatment may be needed. If the misalignment is caught early in a puppy’s life, it may only be temporary and may correct itself over time. However, there are times when intervention may be needed. If your puppy’s teeth are stopping the normal growth of his jaws, then surgery to remove those puppy teeth may be performed. This may allow the jaws to continue to grow, but will not make them grow. For older dogs who are experiencing pain and trauma due to misaligned jaws and teeth, oral surgery is generally performed to extract teeth that are causing trauma, to move teeth so that they fit, or to create space for a misaligned tooth to occupy. Other therapies include crown reductions or braces.
If your dog is genetically programmed to have an overshot or undershot jaw, intervention can help, but will not slow or stop the abnormal growth of either jaw. Prevent jaw misalignments in puppies by not breeding dogs who have overshot or undershot jaws.

You can download this article on puppy teeth problems as an ebook free of charge (and no email required) through the link below. This comprehensive article covers such topics as malocclusions, overbites, underbites and base narrow canines in dogs. Special emphasis is placed on early intervention – a simple procedure such as removing retained puppy teeth can save many problems later on.
One of the biggest misconceptions is that dental problems don’t need the same treatment in animals as they do in humans. Nothing could be further from the truth! Dogs’ teeth have the same type of nerve supply in their teeth as we do, so anything that hurts us will hurt them as well.
All dogs, whether they are performance dogs or pets, deserve to have a healthy, pain-free mouth. Oral and dental issues frequently go undiagnosed in dogs, partly because the disease is hidden deep inside the mouth, and partly because dogs are so adept at hiding any signs of pain. As a pack animal, they don’t want to let the rest of the pack (including us!) know they have a problem, as anything that limits their usefulness to the pack may be grounds for exclusion. This is a survival instinct. Dogs will suffer in silence for as long as they can, and they only stop eating when they cannot bear the pain any longer.
This article has been written to help you understand how oral and dental problems develop in puppies, what the implications of these issues are, and what options are available to you and your pup to achieve the best outcomes in terms of overall health, comfort and performance. You don’t need to read it from top to bottom, as your dog would need to be pretty unlucky to need all the advice included here!
However, I do recommend that you look through the information on what a ‘normal’ mouth is, as this will help you to understand how each problem can arise.
If you would like to speak to me for advice on your dog, please feel very welcome to call me on 1300 838 336, or you can email me on support@ sydneypetdentistry.com.au.
baby) teeth which erupt between 3-8 weeks of age. These are replaced by the adult (permanent) teeth between 4-7 months of age. Adult dogs should have a total of 42 teeth. The difference in the number of deciduous and adult teeth arises because some adult teeth (the molars and first premolars) don’t have a deciduous version.
The ‘carnassial’ teeth are the large specialised pair of teeth towards the back of the mouth on each side, which work together like the blades of a pair of scissors. The upper carnassial is the fourth premolar, while the lower one is the first molar The upper jaw is the maxilla, and the lower jaw is the mandible.
The way the teeth align with each other is referred to as the ‘occlusion’. Normally the upper incisors sit just in front of the lower incisors, this is called a ‘scissor bite’. The lower canines sit in the gap between the upper canines and corner (third) incisors, without rubbing against either of these teeth.
Although a scissor bite is standard for most breeds, in some breeds with a short, wide muzzle (brachycephalic skull type), a reverse scissor bite is accepted as the breed standard, where the upper incisors are behind the lower ones, and the lower canines are shifted forward. A level bite (where the upper and lower incisors are in line with each other) is also acceptable in some breeds.
The bulk of the tooth is made up of dentine (or dentin), a hard bony-like material with tiny dentinal tubules (pores) running from the inside to the outside. In puppies, the dentine is relatively thin, making the tooth more fragile than in an older dog. The dentine thickens as the tooth matures throughout life.
The crown is covered in enamel, which is the hardest material in the body (even harder than bone!). This is only made prior to eruption, and cannot be regenerated if damaged.
Inside the tooth is the pulp, which is living tissue containing blood vessels, nerves and immune cells. The nerves have processes which extend through the dentinal tubules, and if these are exposed or stimulated they can cause sensitivity or intense pain.
Malocclusion is the termed used for an abnormal bite. This can arise when there are abnormalities in tooth position, jaw length, or both. The simplest form of malocclusion is when there are rotated or crowded teeth. These are most frequently seen in breeds with shortened muzzles, where 42 teeth need to be squeezed into their relatively smaller jaws. Affected teeth are prone to periodontal disease (inflammation of the tissues supporting the teeth, including the gums and jawbone), and early tooth loss.
Crowded upper incisor teeth in an English Bulldog, with trapping of food and debris. There is an extra incisor present which is exacerbating the problem.
Anterior (rostral) crossbite occurs when one or more upper incisors are positioned behind their lower counterparts. Constant striking of the lower incisors and oral tissues by the upper teeth may result in periodontal disease, pulpitis (inflammation of there sensitive living pulp tissue inside the teeth) and early tooth loss
‘Base narrow’ canines (Linguoverted or ‘inverted’ canines) are a relatively common and painful problem in Australian dogs. The lower canines erupt more vertically or ‘straight’ than normal (instead of being tilted outwards), and strike the roof of the mouth. This causes pain whenever the dog chews or closes its mouth, and can result in deep punctures through the palatal tissues (sometimes the teeth even penetrate into the nasal cavity!). In our practice in Sydney, we see this most commonly in Staffordshire Bull Terriers and Labrador Retrievers.
Lance’ canines (Mesioverted, hard or ‘spear’ canines) occur when an upper canine erupts so it is pointing forward, like a tusk. This is seen most commonly in Shetland Sheepdogs, and can lead to lip trauma and displacement of the lower canine tooth (which cannot erupt to sit in its normal position in front of the upper canine).
Class II malocclusions (‘overshot’) arise when the lower jaw is relatively short compared with the upper jaw. This type of occlusion is NEVER considered normal and can result in significant and painful trauma to the upper gums, hard palate and teeth from the lower canines and incisors.
Class III malocclusions (‘undershot’, ‘prognathism’) occur when the lower jaw is relatively long compared with the upper jaw. The upper incisors may either meet the lower ones (level bite) or sit behind them (reverse scissor bite). While this is very common, and considered normal for some breeds, it can cause problems if the upper incisors are hitting the floor of the mouth or the lower teeth (similar problems to rostral crossbite). If the lower canines are striking the upper incisors, the accelerated dental wear often results in dead or broken teeth.
Class IV malocclusions (‘wry bite’) occur when there is a deviation of one or both jaws in any direction (up and down, side to side or front to back). These may be associated with mild to severe problems with chewing, damage to teeth and oral tissues, and chronic pain.
Normal development of the teeth and jaws is largely under genetic control, however environmental forces such as nutrition, trauma, dental interlock and other mechanical forces can also affect the final outcome.
As the interaction between these factors can be quite complex, it is recommended that you have your pup individually assessed – feel welcome to call me for advice.
Most malocclusions involving jaw length (skeletal) abnormalities are genetic in origin. We need to recognise this as it has enormous implications if you are planning to breed, as once a malocclusion is established in a line, it can be heartbreaking work to try and breed it back out.
The exact genes involved in jaw development are not yet well understood. We do know that the upper and lower jaws grow at different rates, at different times, and are under separate genetic control. In fact, the growth of one only affects the growth of the other if there is physical contact between them via the teeth. This contact is called ‘dental interlock’.
When the upper and lower teeth are locked against each other, the independent growth of either jaw is severely limited. This can occasionally work in the dog’s favour, for example if the lower jaw is slightly long compared with the upper jaw, the corner incisors may lock the lower canines in position behind them, limiting any further growth spurts of the lower jaw.
However, in many cases, dental interlock interferes with jaw development in a negative way. A classic example we see regularly in our practice is when a young puppy has a class II malocclusion (relatively short lower jaw) and the lower deciduous canines are locked behind the upper deciduous canines, or trapped in the tissues of the hard palate. In these cases, even if the lower jaw was genetically programmed to catch up to the upper jaw, it cannot physically do so.
Early removal of the lower canines (and often the lower incisors as well) to relieve this problem is strongly recommended. This procedure is called ‘interceptive orthodontics’ as we are ‘intercepting’ the developing problem before growth is completed and it is too late.
Extraction of these teeth will not stimulate jaw growth, but will allow it to occur if nature (ie genetic potential) permits. It also relieves the painful trauma caused by the teeth to the hard palate whenever the pup closes its mouth (and we all know how sharp those baby teeth are!!). More information on interceptive orthodontics can be found later in this book.
In some breeds, a genetic tendency for retained deciduous teeth can also contribute to the development of problems, such as anterior crossbite seen in several of the toy breeds.
It is crucial to remember that genetic malocclusions are not usually seen in all puppies in an affected litter as they are not dominant traits. Puppies can carry the genes contributing to genetic faults without showing any physical signs at all. If an affected puppy is noted, extreme caution should be exerted when planning future breeding from the parents and siblings, and neutering of the affected puppy is strongly recommended.
Although diet often gets the blame for development of malocclusions, the role of nutrition is actually much less significant than is often believed. Obviously gross dietary deficiencies will affect bone and tooth development, for example severe calcium deficiency can lead to ‘rubber jaw’. However, the vast majority of puppies are on balanced, complete diets and have adequate nutrient intake for normal bone and tooth development.
One myth I have heard repeated by several owners is that strict limitation of a puppy’s dietary intake can be used to correct an undershot jaw. This is simply NOT true. Limiting calories will NOT slow the growth of the lower jaw relative to the upper jaw (both jaws receive the same nutrient supply). Such a practice is not only ineffective, it can be detrimental for the puppy’s overall growth and development.
Trauma, infection and other mechanical forces may affect growth and development of the jaws and teeth. Developing tooth buds are highly sensitive to inflammation and infection, and malformed teeth may erupt into abnormal positions (or not erupt at all!). Damage to developing teeth can also occur if the jaw is fractured.
Retained or persistent deciduous (puppy) teeth can also cause malocclusions by forcing the erupting adult teeth into an abnormal position. As previously mentioned, this may be a genetic trait, but can also occur sporadically in any breed of dog.
A full bite assessment can help differentiate between malocclusions which are due to shifting of teeth alone, and those which have an underlying genetic basis. Contact me if you would like to arrange a bite assessment for your puppy
The basic rule is that every dog deserves a pain-free, functional mouth. If there is damage occurring to teeth, or oral tissues, we need to alleviate this, to allow the dog to live happily and healthily. If there is no functional problem and no trauma occurring, then treatment is simply not required.
Sometimes the hardest part is determining whether the problem is in fact causing pain. As we know, dogs are very adept at masking signs of oral pain, and will and will continue to eat despite real pain. Puppies, in particular, don’t know any better if they have had pain since their teeth first erupted very early in life.
Early assessment to determine whether intervention is required is critical in puppies with any signs of occlusal problems. Not only does this allow us to relieve their pain promptly, it can allow for easier correction of problems than if we wait until the permanent teeth have fully erupted and settled into place.
The overriding aim is always to give the dog a healthy, pain-free and functional mouth. Sometimes this will result in a ‘normal’ mouth, whereas in other cases, this might not be realistically achievable.
While some basic advantages and disadvantages of the different treatment options are outlined here, it is very important to seek specific advice for your individual dog, as no two mouths are exactly the same, and an individual bite assessment will help us determine the best course of action together. You can contact us anytime.
Malpositioned teeth may be moved into a more appropriate position using orthodontic appliances such as braces (yes, braces), wires, elastic (masel) chains or plates (similar to those used in humans!). In some cases, this may be a multi-step procedure which means repeated general anaesthetics.
Extraction of lower canine teeth – the roots of these teeth make up about 70% of the front of the jaw, and so there is a potential risk of jaw fracture associated with their removal. Some dogs also use these teeth to keep the tongue in position, so the tongue may hang out after extraction.
Extraction of teeth may severely limit an animal’s success in the show ring, especially in breeds where the correct number of teeth is emphasised in the breed standard.
Orthodontic movement of teeth is a complicated science, and, while some procedures appear quite straightforward, permanent damage to teeth and the surrounding structures can result from inappropriate procedures, poorly fitted appliances, or excessive pressures.
The outdated practice of using rubber bands to move the teeth is not recommended, as they slip down between the tooth and the gum, causing damage to the sensitive tissue here. The forces applied are also difficult to regulate, which can cause damage to the ligaments around the teeth, as well as the tooth roots. Much safer and more effective methods are now available.
Procedures to alter the shape of the teeth and make them fit better in the mouth can also be performed. This may vary from removal of small amounts of enamel (odontoplasty) to create space between teeth, right through to shortening the crown of a tooth to prevent it from causing trauma (crown reduction).
Crown reduction is commonly performed to treat base narrow canines, or class II malocclusions, where the lower canines are puncturing the hard palate. Part of the tooth is surgically amputated, a dressing inside the tooth to promote healing and the tooth is sealed with a white filling (just like the ones human dentists use). This procedure MUST be performed under controlled conditions as it exposes the highly sensitive pulp tissue. If performed incorrectly, the pulp will become infected and extremely painful for the rest of the dog’s life.
This pup has trauma in the roof of her mouth due to her left lower canine. A crown reduction procedure relieves the trauma while maintaining some functionality and avoiding extraction.
Even the less invasive odontoplasty (enamel shaping) can result in exposure of the sensitive dentine or pulp tissue if taken too far, and must be performed with extreme care to avoid permanent problems. Xrays are recommended prior to surgery so we can measure how far we can go before we get into the ‘danger zone’.
Although sometimes practised, clipping the tips of the teeth of puppies is NOT a humane procedure, and not only causes intense pain (imagine how it would feel if your own tooth was cut in half), but the resulting pulp infection can cause irreversible damage to the adult tooth buds which are developing underneath.
While the dog may lose some function, this is far preferable to doing nothing (this condemns the dog to a life of pain). Indeed, unless released into the wild, dogs do well even if we need to extract major teeth (canines and carnassials), as they have the humans in their pack to do all the hunting and protecting for them.
This is the term we use when we remove deciduous teeth to alter the development of a malocclusion. The most common form of this is when we relieve dental interlock that is restricting normal jaw development. Such intervention does not make the jaw grow faster, but will allow it to develop to its genetic potential by removing the mechanical obstruction.
Extraction of deciduous lower canines and incisors in a puppy with an overbite releases the dental interlock and gives the lower jaw the time to ‘catch up’ (if genetically possible).
As jaw growth is rapid in the first few months of life, it is critical to have any issues assessed and addressed as soon as they are noticed, to give the most time for any potential corrective growth to occur before the adult teeth erupt and dental interlock potentially redevelops. Ideally treatment is performed from eight weeks of age.
Extraction of deciduous teeth is not necessarily as easy as many people imagine. These teeth are very thin-walled and fragile, with long narrow roots extending deep into the jaw. The developing adult tooth bud is sitting right near the root, and can be easily damaged. High detail intraoral (dental) xrays can help us locate these tooth buds, so we can reduce the risk of permanent trauma to them. Under no circumstances should these teeth be snapped or clipped off as this is not only inhumane, but likely to cause serious infection and ongoing problems below the surface.
Permanent enamel damage on adult teeth following extraction od deciduous teeth. The risk of this can be minimised by use of dental x-rays and extremely good surgical technique.
The aim of any veterinary procedure should always be to improve the welfare of the patient, so the invasiveness of any treatment needs to be weighed up against the likely benefits to the dog. Every animal deserves a functional, comfortable bite, but not necessarily a perfect one. Indeed, some malocclusions (particularly those involving skeletal abnormalities) can be difficult to correct entirely.
In addition to the welfare of the individual dog, both veterinarians and breeders need to consider the overall genetic health of the breed. Both the Australian National Kennel Club and (in New South Wales where our practice is situated) the Veterinary Practitioners’ Board stress that alteration of animals to conceal genetic defects for the purpose of improving their value for showing (and breeding) is not ethical.
Vets and responsible breeders work together to improve the conformation of breeds, which can sometimes mean some tough decisions when genetic problems are discovered.
For animals with malocclusions, very strong consideration needs to be paid to whether or not breeding from the affected animal is in the interests of improving the breed. If there is a genetic component, then neutering or selective breeding is recommended. As the vast majority of orthodontic abnormalities are not dominant in their inheritance (not all pups carrying the ‘bad’ genes will have visible problems), a ‘small’ issue seen sporadically can easily become widespread within a line.
This not only means many pups will have physical problems requiring correction for their own individual welfare, but breeding the problem out again can be extremely difficult.
The bottom line is that, while all dogs will have multiple treatment options available, and in some cases the occlusion can be corrected to the point of being ‘good for show’, advice should definitely be sought about the likelihood of a genetic component prior to embarking upon this, as the consequences for the breed can be devastating if such animals (or their close relatives) become popular sires or dams.
Sometimes a tooth is congenitally missing, that is it has never developed. While dogs can physically cope well with missing teeth, in some breeds this is considered a serious fault, and will severely affect the chances of the dog being successful in the show ring.
Alternatively, a ‘missing’ tooth may be unerupted below the gumline. This can only be diagnosed using xrays. In some cases, the tooth may be trapped under a thickened layer of gum tissue, and surgery to relieve the obstruction (an operculectomy) may allow the tooth to erupt smoothly into the correct position if performed early enough.
Impacted lower canines trapped under thick gum tissue. They are also in a base narrow position. These teeth were able to erupt when tissue was surgically released (operculectomy).
Sometimes, the tooth will be in a favourable position but caught behind a small rim of jawbone – again early surgical intervention may be successful in relieving this obstruction. If the tooth is in an abnormal position or deformed, it may be unable to erupt even with timely surgery.
Impacted or embedded teeth should be removed if they are unable to erupt with assistance. If left in the jaw, a dentigerous cyst may form around the tooth. These can be very destructive as they expand and destroy the jawbone and surrounding teeth. Occasionally these cysts may also undergo malignant transformation (ie develop into cancer).
Firstly, if there are two teeth in one socket (deciduous and adult), the surrounding gum cannot form a proper seal between these teeth, leaving a leaky pathway for oral bacteria to spread straight down the roots of the teeth into the jawbone. Trapping of plaque, food and debris between the teeth also promotes accelerated periodontal disease. This not only causes discomfort and puts the adult tooth at risk of early loss, but allows infection to enter the bloodstream and affect the rest of the body.
If the deciduous tooth is still firmly in position as the adult tooth is erupting, it forces the adult tooth into an abnormal position which can cause a significant malocclusion. For example, the lower adult canines normally erupt on the inside of the deciduous teeth, so if they are forced to erupt alongside them, a painful base narrow malocclusion can result.
The upper adult canines normally erupt in front of the deciduous ones, so forcing them further forward can result in ‘lance’ canines. Finally, the upper adult incisors usually erupt behind their deciduous versions, so if these are retained a rostral crossbite may develop.
Retained upper baby canines force the adult canines to erupt in a more forward position. This can close the gap where the lower canine usually sits, forcing it into a traumatic position.
Puppies play rough, chew whatever they can get hold of, and have tiny teeth with very thin walls. Therefore fractures will sometimes occur. A common misconception is that broken deciduous teeth can be left until they fall out. Unfortunately this is NOT true. From the puppy’s point of view, broken teeth HURT, just as they do in children. Anyone who has had a bad toothache would agree that even a few weeks is a long time to wait for relief!
Broken teeth also become infected, with bacteria from the mouth gaining free passage through the exposed pulp chamber inside the tooth, deep into the underlying jawbone. This is not only painful, but can lead to irreversible damage to the developing adult tooth bud, which may range from defects in the enamel (discoloured patches on the tooth) through to arrested development and inability to erupt. The infection can also spread through the bloodstream to the rest of the body. Waiting for the teeth to fall out is NOT a good option!
We cannot rely on dogs to tell us when they have oral pain. It is up to us to be vigilant and watch for signs of developing problems. Train your pup to allow handling and examination of the mouth from an early age. We will be posting some videos of oral examination tips shortly, watch out in your email inbox for this. Things can change quickly – check their teeth and bite formation frequently as they grow.
Seek veterinary care as soon as a potential problem is noticed – you can call me on 1300 838 336 or email me anytime on support@sydneypetdentistry.com.au for advice or assistance.
Remember, early recognition and treatment is crucial if we want to keep your dog happy and healthy in and out of the show ring. The sooner we treat dental problems, the higher the chance of getting the best possible results with the least invasive treatment.
Maintaining a healthy and beautiful smile may be difficult when growing up with an orthodontic issue such as an underbite. Recognizing and correcting underbites is one of the reasons that orthodontists like to see patients by 7 years of age. This is the time when children are still growing and their bones are still immature. Early orthodontic treatment in young children can help to correct difficult problems such as underbites and minimize complicated issues in the future.
An underbite is a malocclusion or “bad bite” that occurs when the lower teeth and jaw protrude beyond the upper teeth and jaw. Underbites can vary in severity from being mild and barely noticeable to being severe enough that there is a distortion of facial features which may create self-esteem issues in the future.
Underbites are typically seen in 5-10% of the general population and usually have a genetic predisposition. If you or someone in your family has an underbite, the likelihood of your child developing an underbite as they grow is high. Some ethnic groups (Asian, First Nations People) are also more likely to develop underbites. Underbites can also occur or worsen due to thumb or digit sucking habits, prolonged pacifier use, a tongue trust, excessive mouth breathing and interferences between upper and lower baby or growing adult teeth.
Each child is unique and the cause of every child’s underbite is not the same. If steps are taken while the patient is young, the right appliance is often just the thing to resolve the problem. This highlights the importance of early orthodontic screening in children, which should be explored by the age of seven. Whether you come to our Sudbury orthodontics or Mississauga orthodontics office, Dr. Virdee will assess the cause and severity of the underbite, and determine the best course of treatment based on the age of the patient.
If the cause of the underbite is due to a problem with the position of the upper or lower front teeth, this is best corrected with limited braces or a removable retainer. However, if the cause of the underbite is due to excessive growth of the lower jaw, this is best treated with an appliance called protraction facemask in combination with a rapid palatal expander. Because your child is still growing, these appliances take advantage of a child’s natural growth potential to correct the underbite without the need for invasive surgery in the future.
A protraction facemask (also known as a reverse pull face mask) is used in combination with an upper jaw expander (rapid palatal expander) to gradually correct the underbite . The expander is inserted first and gently widens the upper jaw (see our treatment of Crossbites to read more about expanders). On the cheek side of the expander, two hooks are used to connect the facemask to the expander with elastics. The facemask rests on the forehead and the chin, which are used as anchors to gently help the upper jaw to grow forward.
Treatment for underbite correction can range from 6 months to a year depending on your child’s growth potential, the severity of the underbite and compliance with wearing the facemask. Because the bones are less mature in younger patients, the upper jaw is easier to grow. If your child has a severe underbite, it makes sense that it will take longer to correct. The greatest predictor however of treatment success is the patient’s compliance or willingness to wear the appliance at least 12-14h per day.
No your child does not have to wear the facemask to school. We ask that you insert the appliance when they get back from school and while they are watching TV and doing homework, or whenever they are at home to maximize the amount of time that they are wearing the appliance. We also ask that the facemask be worn to bed.
Like anything new, your child has to get used to the expander in their mouth. The good news is, because children are more resilient than adults, it’s easier for them to adapt to something new. It usually takes about a week to get used to eating, chewing and speaking with the appliance. When you first start turning the expander, there may be pressure between the two front teeth and a possible gap may develop. We love to see this as orthodontists because this means that the expander is working. Overtime this gap usually closes on its won as the teeth move towards each other. Once facemask therapy is initiated, there may be some pressure on the chin – this is normal and is expected so don’t worry.
The Franklle is a removable appliance that patients can insert and remove on their own. There are several claims that this appliance will help to grow the upper jaw, but recent studies have shown that this is not the case. More often than not, the underbite is corrected by moving the teeth (which is a side-effect of this appliance).
But the underbite is corrected! What’s the difference you ask? The difference is that we didn’t take advantage of the child’s natural growth – we didn’t help the upper jaw grow which is the most important treatment modality that we can use. Remember – moving teeth is easy – but growing bone is very difficult. When you have a patient that has an underbite due to a problem with growth of the jaw bones, its important to use appliances that will address the specific problem and not mask the problem, especially when they are growing.
The chin cup appliance was used commonly in the 60s and 70s although it is seldom used today. It is a device that wraps around the chin and the top of the head to prevent further growth, movement and protrusion of the lower jaw. Again, based on recent studies, the chin cup has shown to be less effecting at doing what it was intended to do. You cannot stop growth of the lower, but you can help the upper jaw to move or grow to compensate for excessive growth of the lower jaw by using a facemask
There are many patients and parents that are looking for an orthodontist in Sudbury or an orthodontist in Mississauga that can help them correct underbites. If a patient is close to puberty, treatment with a facemask will likely achieve limited results. In this case we will usually monitor their growth and proceed with treatment options based on growth that is recorded from year to year. If the patient’s underbite is mild and growth is stable where the lower jaw has not grown excessively within the last year of observation, non-surgical treatment using braces, Invisaglin or lingual braces is usually the best option. Moderate to severe underbites with prominent lower jaws often require surgical treatment to achieve desired results. An in depth discussion on surgical orthodontics can be found here.
To achieve strong oral health and a wonderful smile, your upper and lower jaws need to evenly meet. This allows you to do things like eating and swallowing with ease and avoid some very serious health risks to your jaw, mouth and teeth.
A malocclusion is whenever the upper and lower rows of teeth do not meet. There are three types of malocclusions: overbites, underbites and crossbites. Overbites and underbites are the most common but all three require immediate and thorough orthodontic treatment. It can be tricky to know if you have a severe enough overbite or underbite to warrant orthodontic intervention.
How do you go about fixing your overbite or underbite? How do the treatments differ? What can you expect from the various treatments? As you can imagine, there are a lot of questions that you need answered. To start, let’s review the basics of identifying overbites and underbites. Then, we’ll explore treatment options and the best courses of action with respect to dealing with your malocclusion before the problem worsens.
Just because your upper teeth extend somewhat over your lower teeth, doesn’t necessarily mean you have an overbite. In addition, minor overbites are very common and might not require braces. Overbites that are severe enough to need fixing occur when the upper teeth overlap the bottom teeth to an excessive degree of roughly 4 to 10 millimeters. This can be caused by genetics, a recessive chin, misaligned bites, thumb sucking, poorly fitted crowns, gum disease or as the result of injury. Also, sometimes teeth just come in awkwardly.
Overbites are more common than underbites and are called a Class II bite. One thing to remember is that having a slight overbite is normal because the shape of the human skull naturally allows for the upper teeth to extend beyond the lower teeth. During checkups, your dentist should measure your overbite and underbite and consult with you if they suspect any issues.
The good news is that overbites are considered to be easily treatable using conventional methods. It is easier to fix in young children so don’t hesitate to speak with an orthodontist immediately about your child or children’s potential malocclusion. It’s never too late to fix this issue if the patient is willing.
An underbite, a Class III bite, is when the lower teeth extend beyond the upper. Essentially, the lower jaw protrudes, making it impossible for the lower row of teeth to align with the upper row causing the potential for several serious oral health issues. This can be caused by the upper jaw bone being underdeveloped or the bone in the lower jaw being overdeveloped.
Like overbites, underbites can begin during childhood due to behaviours like thumb-sucking or caused by genetics or as the result of an accident. Whatever the cause, severe underbites should be treated immediately as to avoid the potential hazards that can surface over time.
Most people believe there are only two malocclusions. There is a third type, though, known as a crossbite. And while it is less common, it still requires diagnosis and treatment. Crossbite is a lateral misalignment meaning the top teeth are positioned too close to the cheek or tongue.
Crossbite occurs during childhood and doesn’t naturally correct itself over time. It can occur between the front or back teeth. The side effects are similar to and just as serious as overbites and underbites. Upon diagnosis, your dentist should present treatment options and recommend a course of action.
While you can do a remedial check to see if you exhibit the signs of having a misaligned bite, this is a job best left to your dentist or orthodontist. They will conduct an inspection that looks for:
There are also mental health and self-esteem risks associated with overbites and underbites. This is often overlooked but our appearance can inform how we feel and determine our emotional state. We believe that dentistry should help you feel confident and comfortable with your smile.
For less severe bites, a removable retainer is a suitable enough solution to produce the desired results. This type of retainer hooks around the back teeth to hold itself securely in place. The removable element makes it easier to clean your teeth but the patient must be responsible enough to remember to put it in every day. Forgetting for long stretches would negate this treatment’s effectiveness.
The most common way to treat misaligned bites is with braces or aligners, especially with children or teenagers. Braces use taut wires to connect tiny brackets to apply consistent pressure to teeth. This forces them to realign and straighten over time. Braces have a high success rate but can be pricy and patients must wear them for anywhere between one to three years.
If you need more incentive to deal with a misaligned bite early, keep in mind that insurance providers often cover braces for children but not adults. We always recommend speaking with your insurance provider to discuss your coverage and payment options.
Some cases of misaligned bites only require aligners. Popular options like Invisalign, which are clear and removable, work wonders while allowing people to go about their day with minimal interruption or embarrassment. Invisalign isn’t an appropriate solution for every case of malocclusion so ask your dentist if they make sense for your situation.
Treatment duration depends on the severity of your issue but be prepared to commit for several months if not a year or two. It might sound as if treatment will upend your life but it is worth it for both your oral health and the smile you will achieve and get to show off every day. Your dentist should be well equipped to talk you through the emotional impact of these procedures and help prepare you for any changes to your daily life.
Don’t wait and let your overbite, underbite or crossbite worsen and create additional issues for your mouth, teeth and gums. Letting these problems linger can result in you needing caps, crowns or dental hardware installed. Furthermore, neglect can make them harder to fix down the road.
We hope this article has answered some of your questions about overbites and underbites. If you or your child needs treatment, then remember just about any misaligned bite can be repaired. It’s always better to tackle the problem head-on and immediately.



 8613371530291
8613371530291