
overshot jaw factory

Secondly, the growth of the mandible is rostral from the junction of the vertical and horizontal ramus. If the lower canines are embedded in pits in the hard palate, the normal rostral growth of the mandible(s) cannot take place normally due to the dental interlock caused by the lower canines being embedded in hard palate pits. This can cause deviation of the skull laterally or ventral bowing of the mandibles (lower jaws).
Thirdly, the permanent lower canine is located lingual to the deciduous canine. This means that if the deciduous lower canines are in a poor position it is a certainty the permanent teeth will be worse. See the radiograph below. The deciduous canines are on the outside of the jaws and the developing permanent canines are seen in the jaw as small "hats". It is clear that the eruption path of the permanent canines will be directly dorsal and not buccally inclined as is normal.
The permanent successor tooth is located lingual to the deciduous tooth and wholly within the jaw at this stage. Any use of luxators or elevators on the lingual half of the deciduous tooth will cause permanent damage to the developing enamel of the permanent tooth. See the images below showing canines (and also the third incisor) with extensive damage to the enamel. The radiograph also shows how much damage can occur to the teeth - see the top canine and adjacent incisor. Some severely damaged teeth need to be extracted while other can be repaired with a bonded composite. This damage is avoidable with careful technique using an open surgical approach.
Do not try ball therapy with deciduous (puppy) teeth. There are two main reasons for this. Puppy teeth are fragile and can easily break. More importantly, the adult canine tooth bud is developing in the jaw medial to the deciduous canine tooth (see radiograph above in the puppy section). If the deciduous crown tips outwards the root will tip inwards. This will push the permanent tooth bud further medial than it already is.
The intention of the procedure is to keep the pulp alive and allow the shortened lower canines to develop normally and contribute to the strength of the lower jaws.
The advantage of this procedure is that the whole of the root and the majority of the crown remain. The strength and integrity of the lower jaw is not weakened by the procedure and long term results are very good due to the use of Mineral Trioxide Aggregate as a direct pulp dressing.
However, many owners are concerned (rightly) about the loss of the tooth and the weakness it may cause to the lower jaw(s). It is not our preferred option. This is not an easy surgical extraction and the resulting loss of the root causes a weakness in the lower jaws. This is compounded if both lower canines are removed.
Normally a composite resin bite plane is bonded onto the upper teeth (see below) with an incline cut into the sides. The lower canine makes contact with the incline when the mouth closes and, over time, the force tips the tooth buccally. This takes around four to eight weeks. The lower canine will often migrate back into a lingually displaced position when the bite plane is removed. This can occur if the tooth height of the lower canine is too short (stunted). If the lower canine is not self-retained by the upper jaw when the mouth is shut further surgery may be required.
We do not perform orthodontics in these cases as the condition is most often due to a combination of long lower jaws (relative to the upper jaw) plus excessive crowding of the incisors. The correct term is mandibular mesioclusion or class 3 bite but undershot is the term in common use.
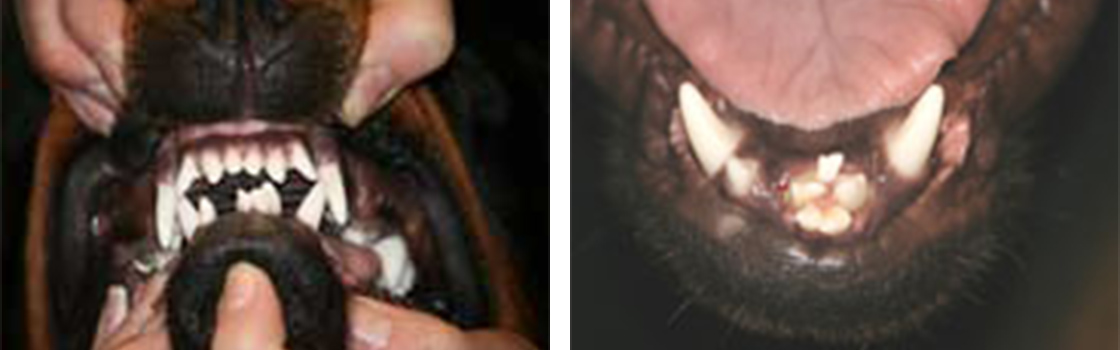
Little Dachshund "Mille" has what is known as brachygnathia inferior- or an overshot jaw. This is where her lower jaw is not as long as her upper jaw.
As she is only a young puppy, it was decided to remove her puppy teeth to remove the pain and then she will be carefully monitored to see if her lower jaw would then "catch up" to her upper jaw.



 8613371530291
8613371530291